Risky Sexual Behaviour Assessment Scale for Young Women:
Development and Psychometric Assessment
Azam Rahmani, Assistant professor, Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
Jamal Asad Mezel, Professor, Department of General Education, College of Education and Languages, Lebanese French University, Kurdistan, Iraq
Leila Allahqoli, Assistant professor, Endometriosis Research Center, Iran University of Medical of Sciences (IUMS), Tehran, Iran
Arezoo Fallahi, (Corresponding author), Assistant professor, Social Determinants of Health Research Center, Research Institute for Health Development, Kurdistan University of Medical Sciences, Sanandaj, Iran
Narges Sadeghi, Department of Nursing and Midwifery, Islamic Azad University, Khorasgan Branch, Isfahan, Iran
Peter Higgs, Department of Public Health, La Trobe University, Bundoora, Australia
Introduction
-
Sexual risk taking behaviours can lead to a number of negative consequences, including damage to romantic relationships, family conflicts, financial concerns, damage to social reputations, health problems and legal disputes.[1] Risky sexual behaviours are the second main cause of HIV transmission in Iran.[2] According to the latest census conducted in Iran, young people make up about 20 per cent (15 million) of the population[3] and they tend to postpone marriage, the only institution that legally permits them to experience sexual activity. In Muslim societies, as is true within some faith traditions,[4] any relationship outside of marriage is culturally, religiously and legally forbidden.[5] However, despite the law, some people begin their sexual activities before marriage.[6] According to some studies, 54–58 per cent of male and female college students had been involved in premarital heterosexual friendships,[7] and 8–12 per cent of female college students have engaged in premarital sexual activity.[8] Also, a study on Iranian youth reported that 27.7 per cent of young people first experienced sexual intercourse at age fifteen; and 68.2 per cent of sexually active teenagers had had at least one risky sexual encounter.[9] While the reports demonstrated the likelihood of there being a rise in risky sexual behaviour,[10] there is no comprehensive sex education that targets youth in Iran. In fact, in the Iranian context, sexual health education and services provide a variety of challenges and obstacles for unmarried youth.[11] Indeed, an increase in premarital sexual relationships and lack of sex education in the Iranian context conspire to cause youth to experience more risky sexual behaviour.
-
Being able to measure risky sexual behaviour is essential for developing more effective interventions to prevent sexually transmitted infections and unplanned pregnancies. Many studies have demonstrated the need for a valid measure regarding sexual behaviour amongst youth.[12]
-
In the international literature, there are different sexual risk assessment scales, such as the High-Risk Sexual Behavior Scale,[13] the Self-Efficacy to Refuse Sexual Behavior Scale,[14] the HIV Risk-Taking Behavior Scale,[15] and the Self-Report Risky Sexual Behaviors Scale.[16] Because of cultural sensitivity issues, very few studies have been conducted in Iran measuring premarital sexual behaviour.[17] The 'Sexual behavioral abstine [sic] HIV/AIDS questionnaire' is a related scale that has been validated in Iran.[18] This study has been used as a self-administered questionnaire. Also, A. Zadeh Mohammadi et al. have developed the Iranian Adolescents' Risk-Taking Behavior Scale.[19] These two questionnaires focus specifically on abstinence and intention to engage in sexual behaviours and do not include risky sexual behaviours and other protective behaviours. Additionally, items in the questionnaires have not been extracted from adolescent or youth experiences and opinions. Since sexuality, especially premarital sexual behaviour, is a culturally based subject, translating and validating available scales from other contexts would not be appropriate for the Iranian culture. It seems it would be more valuable to develop a risky sexual behaviour scale whose items have been extracted from the experiences, perceptions and viewpoints of youth to assess risky sexual behaviours more appropriately. The aim of this study is to develop and examine the psychometric properties of a risky sexual behaviours assessment scale within the Iranian context. The results of this research provide qualitative data regarding premarital sexual relationships within the Iranian context as well as a valid and reliable measurement to use in future investigations and to improve women's sexual health by implementing appropriate interventions.
Methods
-
The present study was an exploratory mixed method investigation. It was conducted in two phases in 2015. In the first phase, a qualitative approach was applied in order to generate items and develop the questionnaire and in the second phase, the psychometric properties of the questionnaire were assessed.
Phase 1: Item generation and scale development
-
In this phase, a qualitative method and content analysis were used to develop a risky sexual behaviour scale in young women. We recruited a group of young women (n = 33) aged 18–34, who volunteered to participate in the study. Because we intended to explore predominant social and cultural beliefs and extract potential informants for individual interviews, we employed focus group discussions as the primary means of data collection. The sessions were facilitated by defining risky sexual behaviours and using a semi-structured inventory that began with an open ended question, such as: 'What are the risky sexual behaviours among single women?' Afterwards, based on the responses obtained from the participants, subsequent questions were added. The participants with different levels of religiosity challenged each other's viewpoints. We documented our analytic ideas by memo writing. The focus group discussions enabled the investigators to identify potential informants for individual interviews. Those women who had experienced premarital sexual activity were identified during FGDs and invited for individual interviews (four out of the original 33 participants). Although, women who had had premarital sexual experiences did not speak openly in the discussions, we identified these women when they spoke about their beliefs. For example, some of them believed that premarital sexual experience is a natural phenomenon and women, like men, could enjoy it. Also, in order to have access to other young women with premarital sexual experiences, snowball sampling was used and an additional eight young females were identified for individual interviews. Sampling was continued with maximum variation to yield greater transferability of data and saturation.[20] To achieve maximum variation, informants were purposively sampled to include different age groups, different socioeconomic backgrounds, various types of sexual experiences, and high and low levels of religiosity. Individual interviews provided a situation for them to speak more deeply about their beliefs and private experiences. Participants had varying educational levels with most living in college dormitories, although a few of them were living with their families at the time of the interviews. Six focus group discussions were held and twelve participants were interviewed individually. Data saturation was achieved after five focus group discussions and 11 individual interviews.
-
We employed qualitative content analysis using an approach developed by Ulla Graneheim and B. Lundman.[21] Data analysis commenced during the data collection process. Each focus group discussion and individual interview was transcribed verbatim and analysed before the next focus group discussion or interview. We achieved thorough comprehension of the data by reading and re-reading. In the next step, the units of meanings were extracted from the statements we had collected. Data analysis proceeded using line-by-line coding; codes were created during repeated discussions between researchers. Categories and themes were created based on the codes with similar meanings. There was an expert second coder in the study. Member checking was completed with five participants who reviewed the summary of the interview data. The substantive codes and themes were also checked with three qualitative data analysis experts.[22] Data collection using multiple methods (individual interview and focus group discussion) enhanced the credibility and dependability of the data.[23]
-
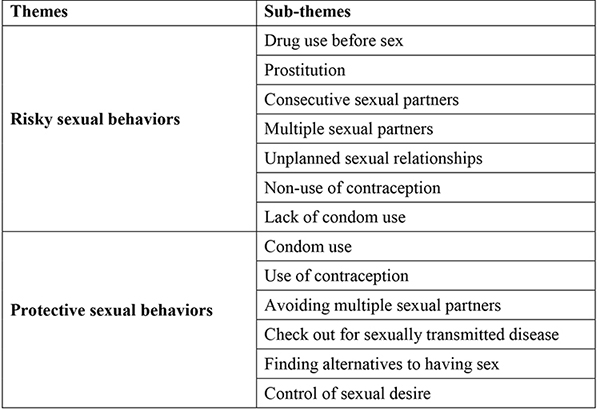
In total, two key themes and 13 sub-themes emerged from the qualitative phase. The framework is shown in Table 1. Finally, an item pool containing 13 statements was generated and has been used for psychometric evaluation.
Table 1. Themes and sub-themes identified in the qualitative phase (phase 1)
Phase 2: Psychometric evaluation of the Risky Sexual Behavior Assessment Scale in young women
-
The pre-final draft of the Risky Sexual Behavior Assessment Scale for Young Women (RSBAS-YW) contained seven items and each item was rated on a five-point response scale (completely agree to completely disagree). A sample of young women aged 18–34 who had engaged in premarital sexual behaviour was recruited from university campus and dormitories. The sample size was estimated based on the number of items in the questionnaire multiplying by 10, as recommended for developing factor analysis.[24] Thus a sample of 70 young women who had experienced premarital sexual relationships was considered optimal. However, given the culturally sensitive information required, there was a risk that we would receive some incomplete questionnaires and so 85 young women were approached and completed the questionnaire. The demographic characteristics of the young women, including age, education and occupational status, were recorded. Several statistical methods were used to analyse the data.
Validity
-
We assessed content, face, and constructed the validity of the Risky Sexual Behavior Assessment Scale for Young Women (RSBAS-YW) as follows:
Content validity
-
Qualitative and quantitative content validity were applied. An expert panel consisting of a team of ten investigators who specialised in sexuality and psychometric evaluation assessed the content validity of the questionnaire. In the qualitative phase, they evaluated wording, grammar, item allocation and the scaling of the questionnaire. In the quantitative phase, the content validity index (CVI) and the content validity ratio (CVR) were calculated. The clarity, simplicity and relevance of each item were assessed by the CVI evaluation process.[25] The CVI was calculated based on the proportion of items that received a rating of 3 or 4 by the experts.[26] The essentiality of the items was tested by calculating the CVR; in fact, the experts rated each item as essential, useful but not essential, or not essential.[27]
Face validity
-
Qualitative and quantitative methods were applied to evaluate face validity. In the qualitative phase, ten young women were asked to evaluate the questionnaire and indicate if they felt any difficulties or ambiguities in formulating their responses. In the quantitative phase, the impact score (frequency × importance) was calculated to indicate the percentage of young women who identified an item as important or quite important. Items were considered appropriate if they had an impact score equal or greater than 1.5, corresponding to a mean frequency of 50 per cent and a mean importance of 3 on the 5-point Likert scale.[28]
Construct validity
-
Exploratory factor analysis (EFA) was used to determine the underlying constructs of the questionnaire. A principle component analysis (PCA) with a varimax rotation was applied and a factor loading equal to or greater than 0.4 was considered acceptable.[29]
Reliability
-
Cronbach's alpha coefficient was calculated to assess the internal consistency of the questionnaire. Values equal to or greater than 0.70 were considered satisfactory.[30] In addition, in order to assess the questionnaire's stability, a test-retest reliability was conducted. Thirty participants completed the questionnaire twice with a two-week interval. The values of 0.40 or higher were considered satisfactory (r ≥ 0.81–1.0 as excellent, 0.61–0.80 very good, 0.41–0.60 good, 0.21–0.40 fair, and 0.0–0.20 poor).[31]
-
Approval to conduct the study was granted by the Ethics Committee of the Faculty of Medicine of Tarbiat Modares University, Tehran, Iran. The participants were informed that participation in the study was voluntary, their confidentiality would be maintained, and none of the participants would be identified in any publications arising from the study. Informed written consent was obtained from all participants.
Results
Participants
-
In total, 85 young women who engaged in premarital sexual relationships were approached. All participants completed the questionnaire and were included in the analysis herewith presented. The mean age of participants was 24.3 ± 3.2 years; and most (68%) were living in dormitories. The characteristics of the study participants are shown in Table 2.
Table 2. Demographic characteristics of the study sample (phase 2, n = 85)
Validity
Content validity
-
In assessing the quantitative content validity, items with CVR and CVI less than 62 and 80,[32] respectively, were omitted; therefore, three items were deleted in this part of the validity process. In the qualitative phase, some criteria such as grammar, wording and item allocation were edited according to the experts' opinions. For example, the sentence 'I have a sexual relationship with someone who has multiple sexual partners' was changed to 'I have sexual relationships with someone who has other sexual partners'.
Face validity
-
The impact score was calculated to examine the quantitative face validity. Impact scores of the items ranged from 1.2 to 5. Therefore, three items with values of less than 1.5 were omitted and seven items were preserved for the next steps of the psychometric assessment. In assessing the qualitative face validity, participants stated that they had had no problems in reading and understanding the items.
Construct validity
-
The exploratory factor analysis (EFA) was used to evaluate the construct validity. The Kaiser-Meyer-Olkin (KMO) and Bartlett's test illustrated that the data were proper for factor analysis (KMO index, 0.71, χ2 = 115.785, P = 0.000). Principal component analysis with varimax rotation identified two factors with eigenvalues greater than 1.5 and a factor loading equal to or greater than 0.4; accounting for 63.1 per cent of variance (Table 3). The factor loadings were as follows.
Factor 1: Protective sexual behaviours that included 4 items, 4, 5, 6, and 7.
Factor 2: Risky sexual behaviours that included 3 items, 1, 2, and 3.
Table 3. Specific values of the total variance explained
Extraction Method: Principal Component Analysis.
-
The final 7-item RSBAS-YW contained two subscales such as protective and risky sexual behaviours. Items in the 'protective sexual behaviours' subscale contained four questions about using condoms, discussing and convincing her/his partner to use condoms, using contraception, and checking for sexually transmitted infections after having a sexual relationship with a new partner. Since these items mostly focused on protective behaviours against sexually transmitted infections or unwanted pregnancy, the title 'protective sexual behaviours' was chosen for this subscale. Also, there were three items in the 'risky sexual behaviours' subscale that included having more than one sexual partner, having sexual relationships with someone who has had more than one sexual partner, and having consecutive sexual partners.
-
The first draft of the questionnaire included some items such as 'receiving money or gifts instead of having sexual relationships' and 'using alcohol or drugs before sexual relationships'; these items were omitted in the process of content and face validity. In fact, in the focus group discussions and individual interviews, few young women who had engaged in typically risky sexual behaviours reported receiving money or using alcohol or drugs before their sexual relationships but these items were omitted because they did not get values more than the acceptable threshold in the validity process. Indeed, these kinds of behaviours were seen in people who engaged in typically risky sexual behaviours but they were not common in young women in general. The results are shown in Table 4.
Table 4. Exploratory factory analysis of the RSBAS-YW*
*Figures in bold are related to factors loaded equal to or greater than 0.4
Reliability
-
Internal consistency was used to evaluate the reliability of the questionnaire. The Cronbach's alpha coefficient for the questionnaire was 0.75, above the acceptable threshold. In addition, the ICC for the questionnaire was found to be 0.87 (good to excellent),[33] lending support to the stability of the questionnaire.
Discussion
-
The results of the present study showed that the RSBAS-YW provided acceptable validity and reliability for accessing risky sexual behaviours in young women. In fact, the CVI and the CVR indicated a reasonable content validity and the Cronbach's alpha coefficient and the results of the test re-test were acceptable and indicated satisfactory reliability and stability for the questionnaire.
-
In international studies, different kinds of risk assessment scales have been developed; some of them, similar to the present study, have focused on risky and protective sexual behaviours. For instance, the HIV Risk-taking Behavior Scale (HRBS) has been developed for sexual risk-taking assessment in intravenous drug users.[34] This scale contains 11 items and two subscales, including substance abuse and sexual risk-taking behaviours. Initial analyses of the HRBS indicated that the scale had satisfactory psychometric properties. The HRBS is similar to the RSBAS-YW, but the RSBAS-YW is applicable to young women. Also, the Self-report Risky Sexual Behaviors Scale (SRSB( is another scale that focuses on risky and protective sexual behaviours. It consists of 20 items, such as unprotected sex, condom use and sexual negotiation.[35] Although the SRSB can be used for both young women and men, the RSBAS-YW has been developed for young women only.
-
Many scales have focused on protective behaviours, especially attitudes to condom use among adolescents and youth.[36] Tapash Roy et al., in their study that assessed the psychometric properties of a condom attitude scale among rural-to-urban migrant workers in Dhaka, Bangladesh, found that the Bengali version of the scale had good metric properties for assessing attitudes towards condom use.[37] The RSBAS-YW evaluates the sexual risk and protective behaviours for young women while the condom attitude scales assess only attitudes regarding condom use. Within the Iranian context, the psychometric properties of two questionnaires have previously been evaluated. The Iranian Adolescents Risk-taking Behavior Scale (ARBS) has been developed to assess seven risky behaviours in Iranian adolescents.[38] One subscale is dedicated to premarital sexual relationships and includes four items such as: 'I think when two people have a close emotional relationship, they can engage in physical intimacy'; 'Sexual relationships could strengthen love'; 'I can select various methods of experiencing sexual activity to meet my needs'; and 'If I love someone, I have enough reason to engage in sexual activity'. This subscale has focused on the attitudes of adolescents to premarital sexual relationships and has not previously examined risk or protective sexual behaviours. Premarital sexual relationships within the Iranian context can be considered as 'risky sexual behaviour' primarily because premarital sexual relationships are not culturally acceptable and there are no sexual health services for unmarried youth.[39] In this case the RSBAS-YW may be considered more appropriate for assessing young people's risky sexual behaviours than the ARBS.
-
The current study has some limitations. Topics related to sexuality are relatively personal and private matters[40] as such research on premarital sexual relationships is difficult in the Iranian context because sexual behaviours before marriage are unacceptable and forbidden by law.[41] In the present study, most people were reluctant to initially speak about their sexual experiences; which meant enormous time and energy was spent establishing rapport and trust. Religious and legal considerations meant that more motivated and/or liberally minded young women participated, even though we invited all young women to participate in the study. A major limitation of our study was the fact that we have not tested for convergent or concurrent validity. In addition, most participants (58.8%) were university students. Since all women in this study were Muslim and most of them were educated, further testing is recommended in other populations including those from urban and regional/rural areas, those with different levels of education, and those different religions and variances in religiosity. Further examination, especially for the confirmatory factor analysis for the RSBAS-YW is suggested.
Conclusion
-
The findings of this study provide preliminary evidence for the psychometric properties of the Risky Sexual Behavior Assessment Scale for Young Women (RSBAS-YW). Further research with a more diverse population of young women is needed to establish stronger psychometric properties for the questionnaire.
Acknowledgements
This study was conducted as part of the first investigator's PhD thesis in Reproductive Health, within the Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran. We would like to thank all young women who took time to participate in this study. Funding was provided by the Faculty of Medical Sciences of Tarbiat Modares University. In addition, there were no competing interests by any of the authors in this study. Ethical approval to conduct the study was granted by the Ethics Committee of the Faculty of Medicine of Tarbiat Modares University, Tehran, Iran.
Notes
All URLs in these references were operational when the paper was published.
[1] Babak Moeini et al., 'Effectiveness of an educational program based on the theory of planned behavior for improving safe sexual behaviors intention among addicted males: A quasi experimental study,' International Journal of High Risk Behaviors and Addiction 6(2) 2017: e32432. DOI: 10.5812/ijhrba.32432.
[2] M. Nasirian et al., 'Modeling of human immunodeficiency virus modes of transmission in Iran,' Journal of Research in Health Sciences 12(2) 2012: 81–87.
[3] Iran-SCo, The Overall Results of General Population and Housing Census, 2011.
[4] Heba Kotb, 'Sexuality in Islam,' PhD thesis, Maimonedes University, 2004.
[5] Farideh Khalajabadi Farahani, John Cleland and Amirhooshang Mehryar, 'Associations between family factors and premarital heterosexual relationships among female college students in Tehran,' International Perspective on Sexual and Reproductive Health 37(1) 2011: 30–39. DOI: 10.1363/3703011.
[6] Farahani, Cleland and Mehryar, 'Associations between family factors and premarital heterosexual relationships among female college students in Tehran'; D.B. Kirby, B.A. Laris and L.A. Rolleri, 'Sex and HIV education programs: Their impact on sexual behaviors of young people throughout the world.' Journal of Adolescent Health 40(3) 2007: 206–217. DOI: 10.1016/j.jadohealth.2006.11.143.
[7] M. Saboor-Parsa and A. Tabatabaee, 'Religion, family and sexual behavior in a university population,' Proceedings of the Second Congress on Family and Sexual Disorders, Tehran, Iran, 2005.
[8] Saboor-Parsa and Tabatabaee, 'Religion, family and sexual behavior in a university population'; Masoomeh Simbar, Fahimeh Ramezani Tehrani and Zeinab Hashemi, 'The reproductive health needs of the university students of Qazvin.' Journal of Qazvin University of Medical Sciences & Health Services 28 2003: 5–13 (in Persian).
[9] Mohammad Reza Mohamadi et al., 'Knowledge, attitude and behavior of adolescent boys aged 15 to 18 in Tehran on Reproductive Health,' Fertility and Infertility Journal 4(3) 2002: 237–50.
[10] K. Mohammad et al., 'Sexual risk-taking behaviors among boys aged 15–18 years in Tehran,' Journal of Adolescent Health 41(4) 2007: 407–414. DOI: 10.1016/j.jadohealth.2007.05.003.
[11] M.R. Mohammadi et al., 'Reproductive knowledge, attitudes and behavior among adolescent males in Tehran, Iran,' International Family Planning Perspectives 32(1): 2006: 35–44. DOI: 10.1363/ifpp.32.035.06.
[12] E.P. Salvagni and M.B. Wagner, 'Development of a questionnaire for the assessment of sexual abuse in children and estimation of its discriminant validity: a case-control study,' Jornal de pediatria 82(6) 2006: 431–36. DOI: 10.2223/JPED.1523; A. Avasthi et al., 'Sexual behavior of married young women: A preliminary study from North India,' Indian Journal of Community Medicine 33(3) 2008: 163–67. DOI: 10.4103/0970-0218.39677; Anthony Biglan et al., 'Social and behavioral factors associated with high-risk sexual behavior among adolescents,' Journal of Behavioral Medicine 13(3) 1990: 245–61. DOI: 10.1007/BF00846833.
[13] C.W. Metzler et al., 'The social context for risky sexual behavior among adolescents,' Journal of Behavioral Medicine 17(4) 1994: 419–38.
[14] Self-Efficacy, Sexual Risk 2010.
[15] Shane Darke et al., 'The reliability and validity of a scale to measure HIV risk-taking among intravenous drug users,' AIDS 5, 1991: 181–85.
[16] Janet S. St Lawrence et al., 'Factor structure and validation of an adolescent version of the Condom Attitude Scale: An instrument for measuring adolescents' attitudes toward condoms,' Psychological Assessment 6(4) 1994: 352–59. DOI: 10.1037/1040-3590.6.4.352; E. Goldberg, et al., 'A human immunodeficiency virus risk reduction intervention for incarcerated youth: A randomized controlled trial,' Journal of Adolescent Health 44(2) 2009: 136–45. DOI: 10.1016/j.jadohealth.2008.07.021.
[17] Farahani, Cleland and Mehryar, 'Associations between family factors and premarital heterosexual relationships among female college students in Tehran.'
[18] Fatemeh Rahmati Najarkolaei et al., 'Sexual behavioral abstine HIV/AIDS questionnaire: Validation study of an Iranian questionnaire,' Journal of Education and Health Promotion 3(10) 2014: n.p.
[19] A. Zadeh Mohammadi, A. Ahmadabadi and M. Heidari, 'Construction and assessment of psychometric features of Iranian adolescents' risk-taking scale,' Iranian Journal of Psychiatry and Clinical Psychology 17(3) 2011: 218–25.
[20] Helen J. Streubert and Dona Rinaldi Carpenter, Qualitative Research in Nursing: Advancing the Humanistic Imperative, Philidelphia: Lippincott Williams & Wilkins, 2010.
[21] U.H. Graneheim and B. Lundman, 'Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness,' Nurse Education Today 24(2) 2004: 105–12. DOI: 10.1016/j.nedt.2003.10.001.
[22] Streubert and Carpenter, Qualitative Research in Nursing: Advancing the Humanistic Imperative.
[23] Streubert and Carpenter, Qualitative Research in Nursing: Advancing the Humanistic Imperative.
[24] Eamonn Ferguson and Tom Cox, 'Exploratory factor analysis: A users' guide,' International Journal of Selection and Assessment 1(2): 1993: 84–94. DOI: 10.1111/j.1468-2389.1993.tb00092.x.
[25] Carolyn Feher Waltz and R. Barker Bausell, Nursing Research: Decision Statistics and Computer Analysis, Philadelphia: Fa Davis Co., 1983; Mary R. Lynn, 'Determination and quantification of content validity,' Nursing Research 35(6) 1986: 382–85.
[26] Waltz and Bausell, Nursing Research: Decision Statistics and Computer Analysis.
[27] C.H. Lawshe, 'A quantitative approach to content validity,' Personnel Psychology 28(4) 1975: 563–75.
[28] Y. Lacasse, C. Godbout and F. Sériès, 'Health-related quality of life in obstructive sleep apnoea,' European Respiratory Journal 19(3) 2002: 499–503.
[29] Ferguson and Cox, 'Exploratory factor analysis: A users' guide.'
[30] L.J. Cronbach, 'Coefficient alpha and the internal structure of tests,' psychometrika 16(3) 1951: 297–334.
[31] Barbara Hazard Munro, Statistical Methods for Health Care Research, 5th ed. Philidelphia: Lippincott Williams & Wilkins, 2005.
[32] Lawshe, 'A quantitative approach to content validity.'
[33] Munro, Statistical Methods for Health Care Research.
[34] Darke et al., 'The reliability and validity of a scale to measure HIV risk-taking among intravenous drug users.'
[35] Brent C. Miller, Brad Benson and Kevin A. Galbraith, 'Family relationships and adolescent pregnancy risk: a research synthesis,' Developmental Review 21(1) 2001: 1–38. DOI: 10.1006/drev.2000.0513; M.C. Aalsma et al., 'The impact of delinquency on young adult sexual risk behaviors and sexually transmitted infections,' Journal of Adolescent Health 46(1) 2010: 17–24. DOI: 10.1016/j.jadohealth.2009.05.018.
[36] St Lawrence et al., 'Factor structure and validation of an adolescent version of the Condom Attitude Scale'; Tapash Roy et al., 'Cross-cultural adaptation of the short-form condom attitude scale: Validity assessment in a sub-sample of rural-to-urban migrant workers in Bangladesh,' BMC Public Health 13(1) 2013: 240. DOI: 10.1186/1471-2458-13-240; Marie Helweg-Larsen, 'UCLA Multidimensional Condom Attitudes Scale,' in Handbook of Sexuality-Related Measures, edited by Terri D. Fisher, Clive M. Davis, William L. Yarber and Sandra L. Davis, 162–64, New York: Routledge, 2011; Marie Helweg-Larsen and Barry E. Collins, 'The UCLA Multidimensional Condom Attitudes Scale: Documenting the complex determinants of condom use in college students,' Health Psychology 13(3) 1994: 224–37. DOI: 10.1037/0278-6133.13.3.224; Idalyn S. Brown, 'Development of a scale to measure attitude toward the condom as a method of birth control,' Journal of Sex Research 20(3) 1984: 255–63. DOI: 10.1080/00224498409551224.
[37] Roy et al., 'Cross-cultural adaptation of the short-form condom attitude scale.'
[38] Mohammadi, Ahmadabadi and Heidari, 'Construction and assessment of psychometric features of Iranian adolescents' risk-taking scale.'
[39] Farahani, Cleland and Mehryar, 'Associations between family factors and premarital heterosexual relationships among female college students in Tehran'; M. Motamedi et al., 'Paradoxical attitudes toward premarital dating and sexual encounters in Tehran, Iran: A cross-sectional study,' Reproductive health 13(1) 2016: 102. DOI: 10.1186/s12978-016-0210-4; Mohtasham Ghaffari et al., 'Premarital sexual intercourse-related individual factors among Iranian adolescents: A qualitative study,' Iranian Red Crescent Medical Journal 18(2) 2016: e21220.
[40] Kevin A. Fenton et al., 'Measuring sexual behaviour: methodological challenges in survey research,' Sexually Transmitted Infections 77(2) 2001: 84–92. DOI: 10.1136/sti.77.2.84.
[41] Farahani, Cleland and Mehryar, 'Associations between family factors and premarital heterosexual relationships among female college students in Tehran.'
|